Fasciocutaneous flap was first described by Bengt Pontén (Sweden) in 1981. He showed that longer flaps (3:1) could be harvested in the leg if the underlying deep fascia was included with the cutaneous flaps— ‘Ponten’s superflaps’.
Fasciocutaneous flaps are axial pattern tissue flaps that include skin, subcutaneous tissue and the underlying deep fascia (with its prefascial and subfascial vascular plexus).
When raised with only subcutaneous tissue and not skin, they are referred to as adipofascial flaps and when raised without any skin or subcutaneous tissue, they are called fascial flaps. Following are the various classifications of Fasciocutaneous flaps.
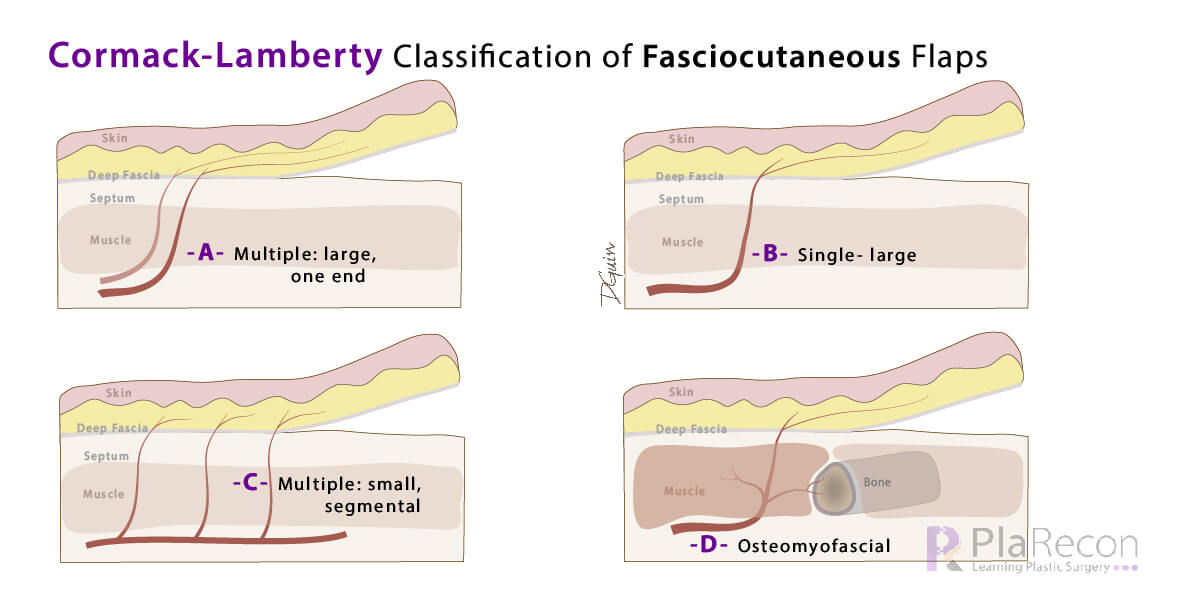
Cormack and Lamberty classification (1984)
Anatomists, G C Cormack, B G H Lamberty (UK), by a series of injection studies, classified fasciocutaneous flaps on the basis of their patterns of vascularisation into 4 types:
- Type A– Multiple fasciocutaneous perforators enter at the base of the flap.
- Eg. Ponten’s ‘superflap’ in the lower limb, Sartorius flap without muscle (Cormack and Lamberty, 1983) and Upper arm flaps based on the medial or lateral intermuscular septum.
- Type B– Single solitary fasciocutaneous perforator supplies the flap. (Modified Type C– Flap islanded based on the single perforator).
- Eg. same as Mathes-Nahai type B below except for radial forearm and peroneal artery flaps.
- Type C– Multiple small perforators in series (segmental) from the main artery supply the skin through the fascial septum (The segment of the main artery with the perforators is included in the flap).
- Eg. Radial forearm flap, Peroneal artery flap.
- Type D– A compound flap including a portion of adjacent muscle and bone- based on multiple small perforators similar to Type-C (osteomyofasciocutaneous).
- Eg. Radial forearm flap with half the diameter of the radius, Fibular flap.
The perforators described above were mainly septocutaneous.
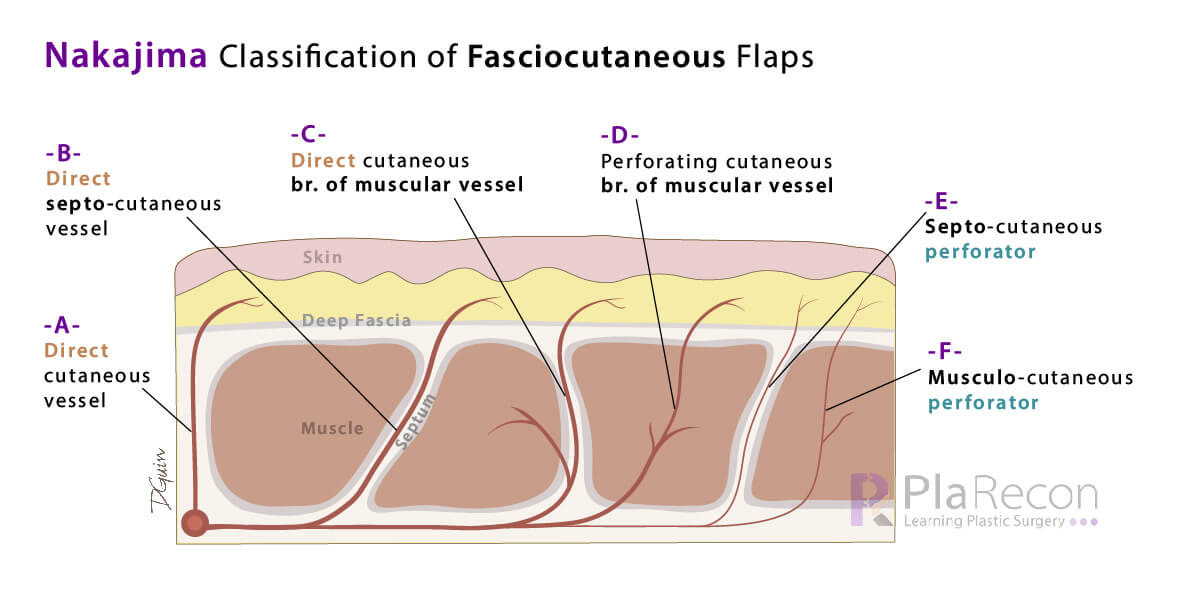
Nakajima classification (1986)
Hideo Nakajima, Toyomi Fujino and Shu Adachi (Japan) further classified fasciocutaneous flaps into 6 types (I – VI) based on the 6 types of deep fascial perforating vessels (A – E):
- Type I– based on Direct cutaneous vessels (type A)- Eg. same as Mathes-Nahai type A below.
- Type II– based on Direct septocutaneous vessels (type B)- Eg. same as Mathes-Nahai type B below.
- Type III– based on Direct cutaneous branch of muscular vessels (type C)
- Type IV– based on Perforating cutaneous branch of muscular vessels (type D)
- Type V– based on Septocutaneous perforators (type E)
- Type VI– based on Musculocutaneous perforators (type F)
Salient points:
- First four vessels patterns (A, B, C, D) had a larger calibre with axial vascular pattern while the latter two (E, F) had a smaller calibre with random vascular pattern.
- Types A, B, C, E were direct perforators to the skin while the other types D, F were indirect (i.e. they traverse through other tissue like muscle, before perforating the fascia and reaching the skin).
- Musculocutaneous flaps were based on these indirect types D, F perforators.
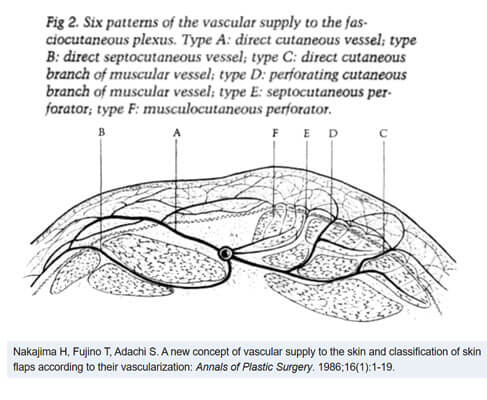
- Flaps III, IV based on C, D were first described by Nakajima et al. and were their most important contribution. Currently, type C is variable and not frequently described, but type D (perforating branch of muscular vessels) is a well-recognized perforator.
Note: The types III, IV based on perforators C and D are labelled differently (interchanged) in some of the popular textbooks. So don’t get confused if the information here doesn’t match with that given there. We have followed the description from the index article by Nakajima et al. (image attached alongside)- Fact checked!
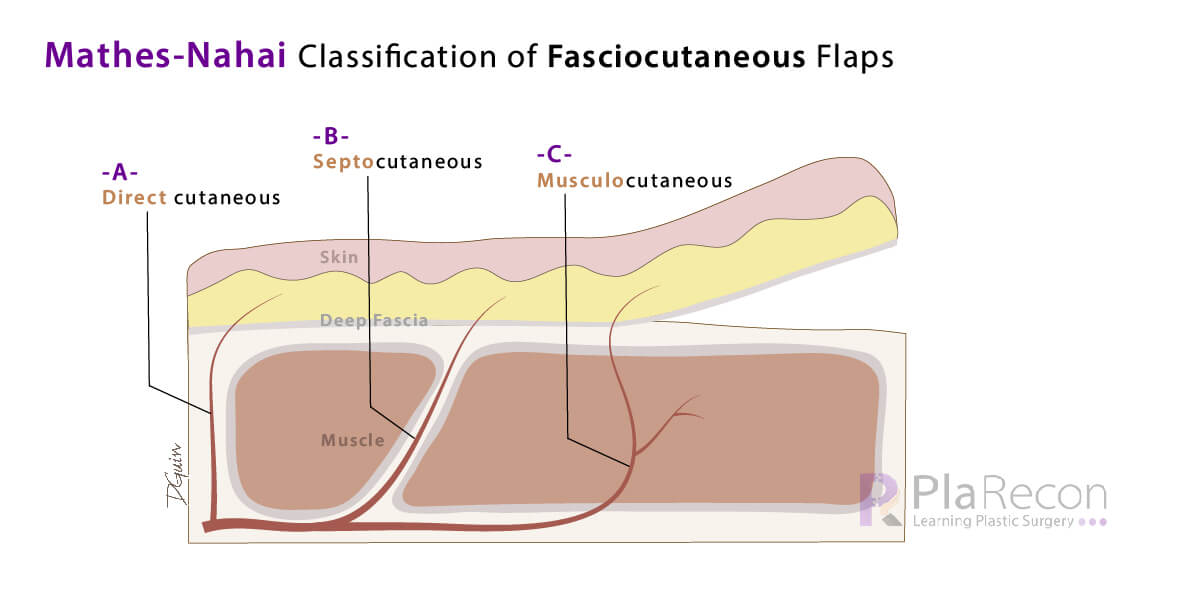
Mathes and Nahai classification of fasciocutaneous flap (1997)
Stephen J Mathes, Foad Nahai (USA) described the simplified tripartite system of fasciocutaneous flaps (3 types) based on the following types of deep fascial perforators:
- Type A– Flap with direct cutaneous pedicle to the fascia.
- Eg. H&N: Scalp, paramedian forehead and temporoparietal fascial flaps; Upper limb: Flaps based on digital and dorsal metacarpal arteries; Trunk: Groin and hypogastric flaps; Superficial external pudendal artery; Lower limb: Gluteal-thigh, pudendal-thigh flaps, sural artery, saphenous flaps and toes for transfer.
- Type B– Flap with a septocutaneous perforator.
- Eg. Trunk: Supraclavicular, scapular and parascapular flaps; Upper limb: Lateral and medial arm, Antecubital, Radial forearm, Radial and ulnar recurrent, PIA (posterior interosseous) flaps; Lower limb: ALT (Antero-lateral-thigh, ATA, Dorsalis pedis, PTA, Peroneal artery, Medial and lateral plantar artery flaps.
- Type C– Flap with perforators from a musculocutaneous source.
- Eg. Median forehead, Nasolabial, Deltopectoral (DP), Thoracoepigastric (transverse abdominal), Transverse back flaps, ALT flaps.
Hope the post and our illustrations helped you remember the fasciocutaneous flap classifications, do subscribe below for more. You may also want to check out some mnemonics for the Mathes and Nahai classification of Myocutaneous flap and also subscribe to our YouTube channel for video tutorials.
References (For further reading):
- Cormack GC, Lamberty BG. A classification of fascio-cutaneous flaps according to their patterns of vascularisation. Br J Plast Surg. 1984 Jan;37(1):80-7.
- Nakajima H, Fujino T, Adachi S. A new concept of vascular supply to the skin and classification of skin flaps according to their vascularization. Ann Plast Surg. 1986;16:1–19.
- Mathes SJ, Nahai F. Flap selection: analysis of features, modifications, and applications. Reconstructive surgery: principles, anatomy, and technique. New York: Churchill Livingstone; 1997. p. 37–160.

Tutorials & tips in Plastic Surgery
+ Weekly updates of high-quality webinars!

{kind=link}
Impressive article with clarity.
Thank you, glad you liked it.
very nice.
Thank you!