Julius H. Jacobson II (Vascular surgeon, USA) in 1960 first used an operating microscope to join 1.4mm diameter vessels and coined the term ‘Microsurgery’. Following this in 1962, Ronald A Malt & Charles F McKhann (USA) performed the first successful replantation (of the arm of a 12-year old boy).
Inspired by them, Susumu Tamai (Japan) began microvascular research in 1964 and eventually (with Shigeo Komatsu) performed the first successful replantation of digit (thumb) in 1965. This created a sensation around the world at that time and in turn inspired some surgeons, who started performing more and more digital replantations in the 1960s and 1970s. Thus, by the end of the 1970s, there was a need to define and classify digit and hand amputations. Some of the fingertip amputation classifications (Allen, Tamai, Ishikawa, Hirase) are mentioned chronologically below.
Elsahy Classification (1977)
Nabil I Elsahy (USA) in 1977 was among the first to make an attempt to classify fingertip amputations. The nail was used as the basis of the classification. The amputated parts were sutured back and their survival was studied.
- Group I – without the involvement of nail.
- Group II – with the involvement of nail.
- IIA – distal to lanula.
- IIB – proximal to lanula.
- IIC – proximal to lanula and distal to DIP joint.
(Group IIC, though described, was not included in the study as their survival chances without microvascular anastomosis was very low)
In the VII Symposium of the International Society of Reconstructive Microsurgery in Brazil (1979), the ‘Replantation Committee’ that included Edgar Biemer (Germany), Paul G Lendvay (Australia), Susumu Tamai (Japan) and James Urbaniak (USA) presented their report (based on a study of the international literature on replantation surgery) which dealt in detail with definitions and classifications in replantation surgery and was published by Biemer in 1980. The amputation at various levels of the hand and digits were classified of which the fingertip amputation classification was similar to the Tamai classification mentioned below.
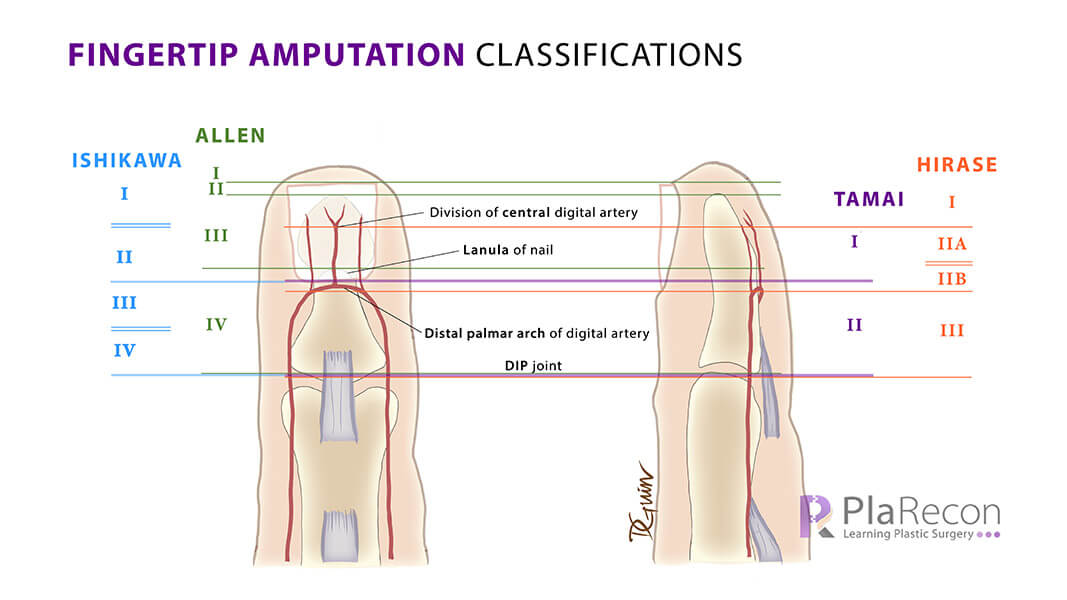
Allen Classification (1980)
The classification by M J Allen (UK) was based on the involvement of pulp, nail (its lanula), and terminal phalanx. All cases were managed conservatively (no replantation was performed) and the deformities, late functional results noted. Allen’s classification is still widely used.
- Type I – only pulp distal to the nail.
- Type II – pulp + part of nail distal to the distal phalanx.
- Type III – pulp + part of nail distal to the lanula + part of terminal phalanx.
- Type IV – pulp + involvement of lanula of nail + part of terminal phalanx.
Tamai Classification (1982)
Susumu Tamai (Japan) put forward an anatomical classification for fingertip amputations, with special reference to the replantation technique. For firgertips, its divided anatomically based on the nail and also the anatomy of the digital arteries. It’s the simple and practical and hence one of the most frequently used classification.
- Zone I – distal to the nail fold (The digital arteries of ulnar and radial sides form an arch and branch into tiny branches in this zone.)
- Zone II – nail fold to distal interphalangeal (DIP) joint
Trivia: As we can see, most of the fingertip amputation classifications are from Japan. What do you think is the reason?
Ishikawa Classification (1990)
Kozo Ishikawa (Japan) classified fingertip amputation around the nail but then based on the vascular anatomy of the fingertip.
- Subzone I – From the tip of the fingertip to the midpoint of the nail.
- In 1997, Naiem S Moiemen & David Elliot (UK) modified Ishikawa Classification by dividing subzone I into:
- IA – from tip of the fingertip to the distal end of the nail (which could be resutured as a composite graft in children).
- IB – from the distal end to the midpoint of the nail.
- In 1997, Naiem S Moiemen & David Elliot (UK) modified Ishikawa Classification by dividing subzone I into:
- Subzone II – From the midpoint of the nail to the base of the nail.
- Subzone III – From the nail base to the midpoint between nail base and the DIP joint.
- Subzone IV – From the midpoint between the nail base and the DIP joint to the DIP joint.
Hirase Classification (1997)
Yuichi Hirase (Japan) used the level of reattachment of amputated part or level of arterial anastomosis during replantation to classify Distal Phalanx (DP) amputations anatomically and provided zone-wise surgical principles:
- Zone DP I – Distal to the most distal dividing point of the central digital artery. (Amputated part is reattached as a composite graft.)
- Zone DP II – includes the distal palmar arch of digital artery and the central digital artery arising from it. (Arterial anastomosis is done in the midline, Venous anastomosis is not done, K-wire is not passed to facilitate venous return through medullary cavity. Digital nerve is sutured if possible). Zone DP II is divided into A, B based on level of anatomosis:
- DP IIA – Arterial anastomosis is done to the central digital artery arising from the distal palmar arch of digital artery.
- DP IIB – Arterial anastomosis is done directly to the distal palmar arch of digital artery.
- Zone DP III – Proximal to the distal palmar arch of digital artery (Digital artery, vein and nerve are anastomosed laterally and axial K-wire passed through terminal phalanx)
References (For further reading):
- Elsahy NI. When to replant a fingertip after its complete amputation. Plast Reconstr Surg. 1977 Jul;60(1):14-21.
- Biemer E. Definitions and classifications in replantation surgery. British Journal of Plastic Surgery. 1980;33(2):164-168.
- Allen MJ. Conservative management of finger tip injuries in adults. Hand. 1980;os-12(3):257-265.
- Tamai S. Twenty years’ experience of limb replantation—Review of 293 upper extremity replants. The Journal of Hand Surgery. 1982;7(6):549-556.
- Ishikawa K, Ogawa Y, Soeda H, Yoshida Y. A new classification of the amputation level for the distal part of the fingers. J Jpn Soc Microsurg. 1990;3:54–62.

Tutorials & tips in Plastic Surgery
+ Weekly updates of high-quality webinars!

{kind=link}
Very interesting to read